Thought this was interesting, somebody was saying there would be a huge financial hit for universities from student drop off. Didn’t happen this year. Assuming by next summer we are in a better spot with the virus and economy, looks like there wont be much of an issue for UH.
Meanwhile , back on the IHME graph, it’s showing
415,000 dead by January 1st.
How about you medical field folks with internal
projections, Are these projections under or over
your internal estimates ?
Good luck solving those “complexi” problems.
1 Like
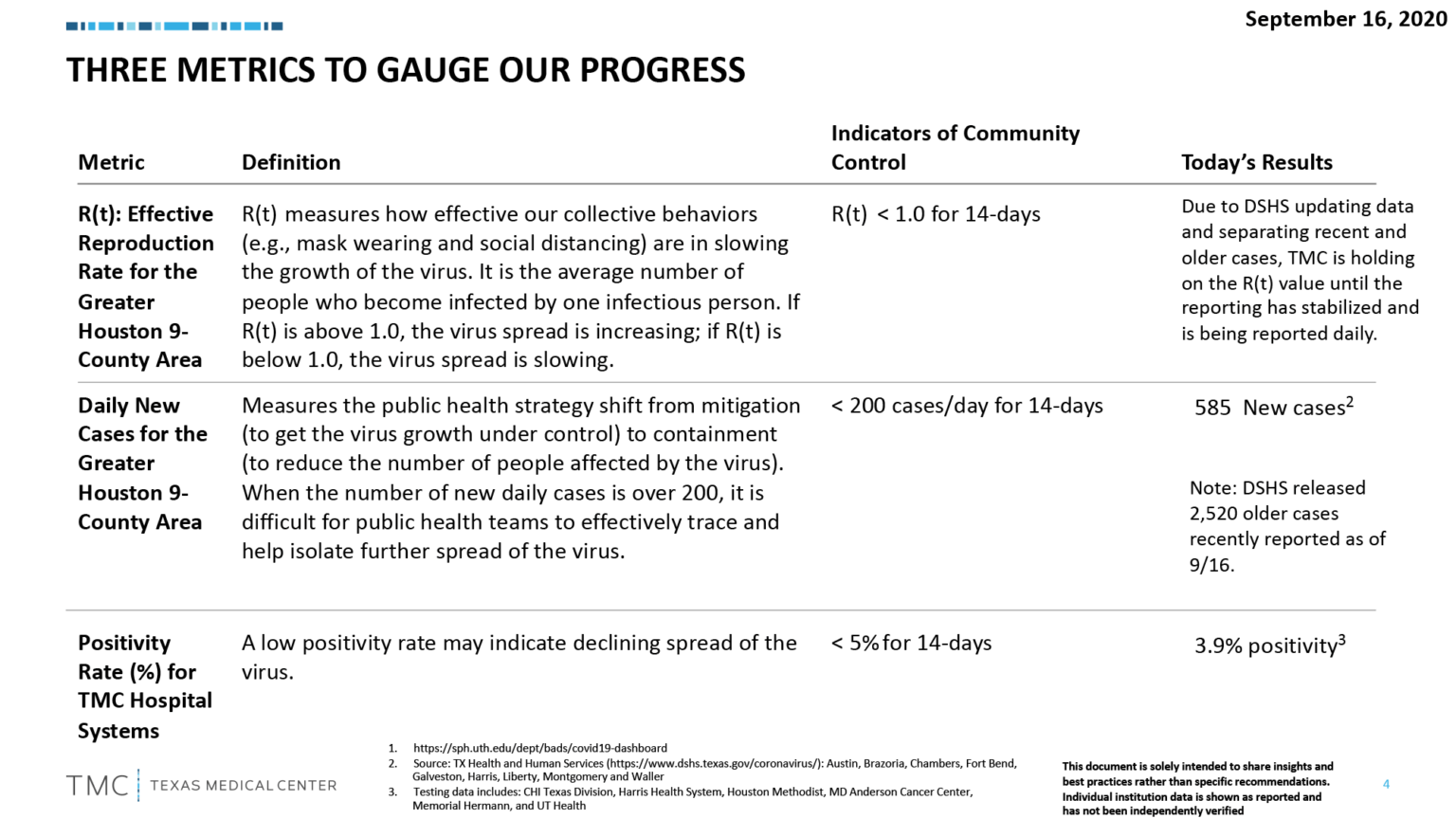
INCREASING CAPACITY: Gov. @GregAbbott_TX said the state will allow restaurants, retail & gyms to expand the 75% capacity. It’s based on percent of COVID-19 patients below 15% in a region. It’s 5% in Houston. This is a change from positivity. Still NO bars
“Its a bold strategy Cotton”
As a completely non medical person, but one who loves statistics and checking out all the projections, I would put big money on the under. Even if things get super bad, I can’t see 164k deaths in November/December like they have projected. I think their projections could be correct in the short term and get us up to near 250k deaths by the end of October, but I can’t see a spike worse than April/May unless NYC has a bad 2nd wave and the rest of the country increases as well.
We (nationally) currently have a slight increase in cases and deaths, if that continues through next week then we might be in trouble.
The idea it would only be 50 percent effective does concern me
If there is another surge, cool weather could be the multiplier that gives the shape of a fall surge a steeper curve than spring/summer surge. This is what a lot of the models are contemplating. We have no way of knowing how COVID will behave in the fall because it’s unprecedented. But we can’t necessarily straight line it based on historical trends either because the drivers are a bit different.
I saw that on the DSHS dashboard, but it said they were not included on the new case numbers so that shouldn’t have impacted the current trend. I saw the national 7 day trend is up some the last few days.
Some people say that by Thanksgiving, you know in theory, when it gets a little colder, it miraculously goes away. I hope that’s true.
I heard it from a waiter, so it must be true.
3 Likes
That is one of the reasons people should have tempered expectations on the efficacy of any vaccine.
With multiple vaccines likely being available it will be important for people to listen to their health care experts and read the PI prescribing information that will be available to read.
Then there is the supply chain logistics challenges as Mystic pointed out.
It will require major refrigeration and likely will not be available at your doctors office any time soon.
People are going to be bummed they will not have their do it home vaccines under the tree in time for Christmas like 23 and me.
Need to keep an eye on Europe.
They say the rise in infections is due to increased testing, but like always, we will see if this is a leading indicator of another surge. Death rates have not risen, but as we all know, there is a lag.
I was watching something the other day and it said that we might not have enough syringes to administer a vaccine and vials to hold the vaccine for a while.
If so, this sounds like something the feds need to take hold of and order production under that War Production Act (or whatever it’s called).
Wouldn’t it be a shame if somebody did find a pretty good vaccine and we’ve got months or years to wait to take it because of supply issues?
1 Like
Even if we flip the War Production Act on tomorrow because a vaccine is ready to be administered to the public, do we have the manufacturing facilities in place to do so in a reasonable amount of time? We’re not producing generic machinery like warplanes or even respirators that can be made out of any run of the mill production facility. If not, have we started building out the facilities on the front end so that we have the capacity when it is time?
I am not a supply chain guy but, yes is my guess. These are some of the issues the the Defense Production Act May be used for I believe. Even down to the alcohol swab that may be used.
It may be accounted for but I have not seen details. I have seen preliminary ideas for distribution but the devil is always in the detail.
This where it would be nice to have a national plan instead of having it be state vs state.
Things I have heard about some of the reasons for the surge in Europe…young people. Young and dumb is not unique to this country.
Here is some new data on viral load and mortality.
Recall what I shared from a recent call about a good fitting mask that may reduce the viral load exposure, thus likely improving outcomes.
Overall, the in-hospital mortality rate was 38.8% among patients with a high viral load, 24.1% among patients with a medium viral load, and 15.3% among patients with a low viral load ( P <0.001)
Here is one of the best descriptions to explain viral load.
In general with respiratory viruses, the outcome of infection – whether you get severely ill or only get a mild cold – can sometimes be determined by how much virus actually got into your body and started the infection off. It’s all about the size of the armies on each side of the battle, a very large virus army is difficult for our immune systems army to fight off.
Your bodies immune system reacts in 2 ways. First, the innate immune response, the generic antiviral response. This the cytokine or Bradykinin storm that illicits the symptoms, it is your body trying to slow down the infection. It’s your bodies response until the acquired response, virus specific defense your body does kicks in.
We haven’t even gotten Texas’s seven day moving average for deaths below 100 yet. It even went back up to 120. Yet we are opening things up further.
How many more days are left in 2020? Now multiply that by 100.
That’s 10,500 more deaths this calendar year alone. Remember when someone posted here that Texas wouldn’t even have 7,000 deaths from COVID?
The saddest thing is we actually undercount deaths. While we currently have over 14,000 officially, we had 19,900 excess deaths from March 15- Aug15. Which means we are well over 20K now.
It’s very disheartening.
4 Likes
Agree, it’s still too early to be opening more things.
Texas is 3rd behind NY and NJ in deaths and at 100/day we will be chasing only NY in about 20 days. Our 7 day trend death total is still at 120/day.
And the fact we are just in the 2nd week of school being in session. It will be 2 more weeks before we
can accurately assess that move, and yet we open up more.
Same play , Act II.
1 Like
Yes, I saw that in a UH communication.
That is remarkable considering all the economic pain that started in the country in March with the economic lockdown that is still being felt and will be felt for quite some time. The general perspective was that universities would be significantly impacted, and enrollment would be down. Would have to check and compare against enrollment across a portfolio of universities to check if that concern came to fruition.
I see the increase is due to added masters programs which is great. But the University experiended a " 7 percent decrease in the number of first-time college students." which they appear to be equating to the virus. Which should be expected and it could be a lot worse. It would still be interesting to see how it equates to universities across the board and how we compared with the 7% decrease apples to apples.
They appear to be, but they are still a mitigation and certainly something almost all of us don’t want to deal with long-term. The vaccines that are being validated and coming out are the problem solvers. Or at least they are expected to be.
I just saw your response. I have been promoting wearing masks since the concept came out in late March for Coranvirus here in the US. It’s the reason why my family have been reinforcing our masks with HEPA approved filters at 99.97% from the early days of mask wearing. We were hoping to improve our mask’s effectiveness and I am pretty sure we have from the average mask out there.
Sure, studies show the effectiveness of masks with infection rate reductions with increased usage of masks in public. But vaccines are being proved in lab environments at the microscopic level with understanding how the vaccines work and how they combat the virus. But have masks of all kinds being worn in public been tested in lab environments and tested the effectiveness rating of masks material with Coronvirus substances being jetted through them in a controlled lab environment to determine their level of effectiveness to two or three decimal places? Maybe one or some are out there, but I have not seen them. I do not need that kind of lab testing to wear my mask out there every day, but I believe the science will be more behind the vaccine than the mask. Until the vaccines have been approved and distributed and I am vaccinated, I’ll continue to wear my masks. There is a big diffrence between being “effective” vs knowing and validating the effectiveness and espeically being proven in a lab ienvironment to 3 decimal places.